
By Karin Elgar
Abstract
Introduction
General Effects
Clinical Uses
Safety
Drug and Disease Interactions
Pregnancy, Breastfeeding and Children
Conclusion
Acknowledgements
References
Abstract
Resveratrol is a polyphenol found in many plant foods, and in particularly high concentrations in red wine. Epidemiological studies have shown significant reductions in all-cause mortality with dietary patterns high in resveratrol, and preclinical research has identified a number of anti-inflammatory, antioxidant, anti-cancer and cardioprotective mechanisms of resveratrol.
Resveratrol has been studied in a number of conditions, including Alzheimer’s disease, cognitive function, cardiometabolic conditions, osteoporosis, autoimmunity and for cancer prevention. For most clinical uses, studies are limited and conflicting results have been observed. The range of dosages used in clinical trials has also varied widely and there are some suggestions of a non-linear dose−response relationship, with high dosages potentially harmful. More clinical research is needed for practitioners to base their recommendations on.
Cite as: Elgar K. (2021) Resveratrol: A review of clinical use and efficacy. Nutr. Med. J., 1 (2): 37-53.
Affiliation: K. Elgar is with the Nutritional Medicine Institute, London, UK.
Article history: Received 10 March 2021. Peer-reviewed and received in revised form 19 August 2021. Accepted 02 September 2021. Available online 14 April 2022.
Published by: The Nutritional Medicine Institute
Open Access: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs licence (http:// creativecommons.org/licenses/by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any medium, provided the original work is not altered or transformed in any way, and that the work is properly cited. For commercial use please contact support@nmi.health
Introduction
Resveratrol is a polyphenol found in a number of plant foods, including red grapes and its products, blackberries, cacao, cranberries, peanuts and pistachios.1 The high resveratrol content of red wine is thought to, in part, explain the ‘French paradox’, that is people in the South of France having a low incidence of coronary heart disease despite high intakes of saturated fat, but also of red wine.2
Since an article in the journal Science in 1997 reported anti-cancer properties of resveratrol,3 a lot of research has focussed on its health effects and relevant mechanisms. Epidemiological studies have shown that dietary patterns high in resveratrol are associated with a significant reduction in all-cause mortality; however, findings from observational studies regarding specific conditions are often inconsistent.4 Preclinical research has identified a large number of mechanisms by which resveratrol exerts anti-inflammatory, antioxidant, anti-cancer and cardioprotective effects.1,4,5
Resveratrol is poorly absorbed, and bioavailability is generally poor due to its rapid conjugation to glucuronic acid and sulphates.2 It is thought that red wine is the most efficient way to ingest resveratrol, although resveratrol content in wine can vary widely.1 Dose−response effects with resveratrol tend to be non-linear, indicating a complex nature of low dietary doses versus high pharmacological doses,2 with higher dosages potentially increasing the risk of adverse effects in patients with cardiovascular disease (CVD).6
The aim of this paper is to review the evidence from clinical trials for the use of resveratrol in clinical practice.
General effects
Antioxidant effects
Many preclinical studies have shown that resveratrol has strong antioxidant effects through a number of pathways, including reducing reactive oxygen and nitrogen species, directly scavenging free radicals, increasing gene expression of the antioxidant glutathione, the antioxidant enzymes catalase (CAT) and superoxide dismutase (SOD), nuclear factor erythroid-2-related factor 2 (Nrf2, which regulates antioxidant pathways) and phase II detoxification enzymes (see figure 1).
Figure 1: Activation of Nrf2 Signaling by Resveratrol
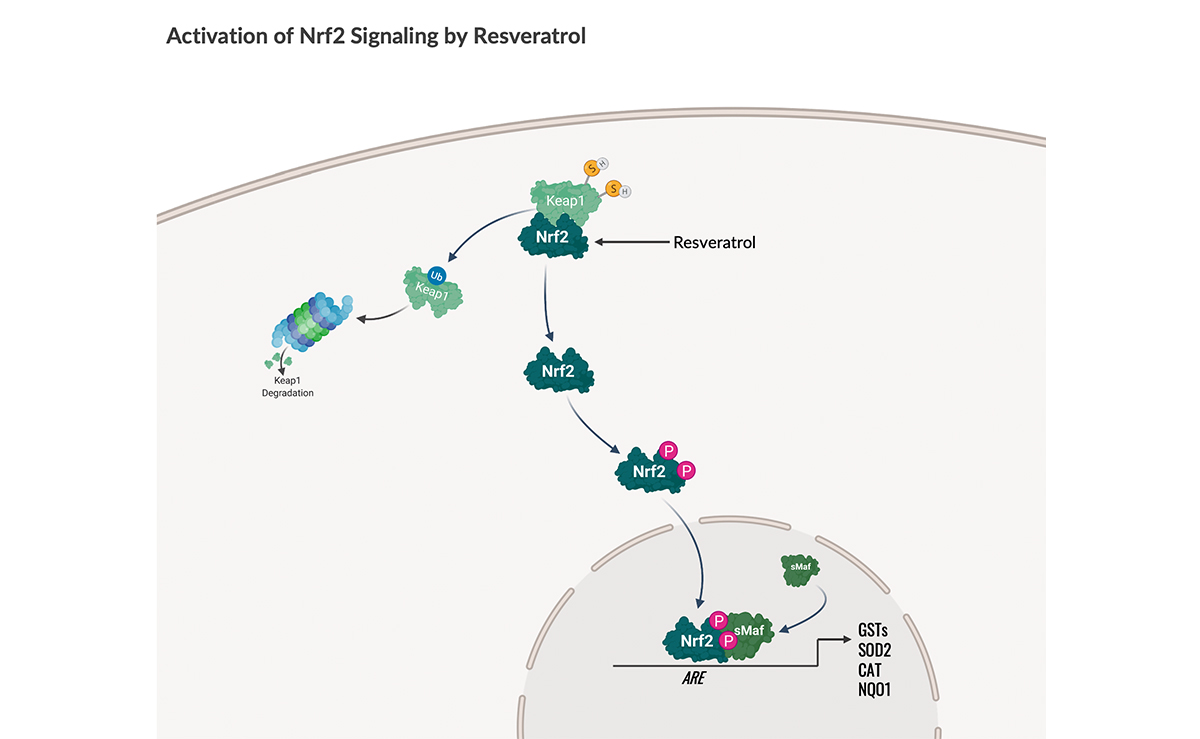
Figure 1; Resveratrol promotes the expression and function of nuclear factor-erythroid factor 2-related factor 2 (Nrf2), a redox-sensing transcriptional activator of antioxidant genes and detoxification enzymes. Under homeostatic conditions, the Nrf2 transcription factor is restrained in the cytosol by Kelch-like ECH-associating protein 1 (Keap1). In the presence of oxidative, chemical, or electrophilic stress, Nrf2 translocates to the nucleus and heterodimerizes with Maf proteins to bind antioxidant response elements (AREs) in the promoters of genes encoding antioxidant proteins, phase II detoxification enzymes and glutathione biosynthetic enzymes. Target genes involved in cellular defenses include glutathione sulfotransferases (GSTs), catalase (CAT), superoxide dismutase 2 (SOD2) and NAD(P)H quinone dehydrogenase 1 (NQO1). Image credit: Kelly Heim, Ph.D. Created with BioRender.com.
Anti-inflammatory effects
Resveratrol activates sirtuin 1 (SIRT1), a protein that plays an important role in the regulation of metabolism and inflammation.2 A clinical trial has shown that over 30 days, resveratrol, 500 mg per day, can increase SIRT1 as much as caloric restriction (1000 kcal per day), which is known for its beneficial effects on inflammation and metabolism.7 However, another clinical trial comparing calorie reduction with resveratrol did not confirm any increase in SIRT1, so more research is needed to explore this effect.8
Resveratrol also regulates the production of pro- and anti-inflammatory cytokines, such as tumour necrosis factor alpha (TNF-α), interleukin-1β (IL-1β) and interleukin-6 (IL-6), and affects nuclear factor kappa B (NF-ĸB), which regulates inflammation and immune responses amongst other inflammatory mechanisms (see figure 2).
Figure 2: Inhibition of NFκB Signaling by Resveratrol
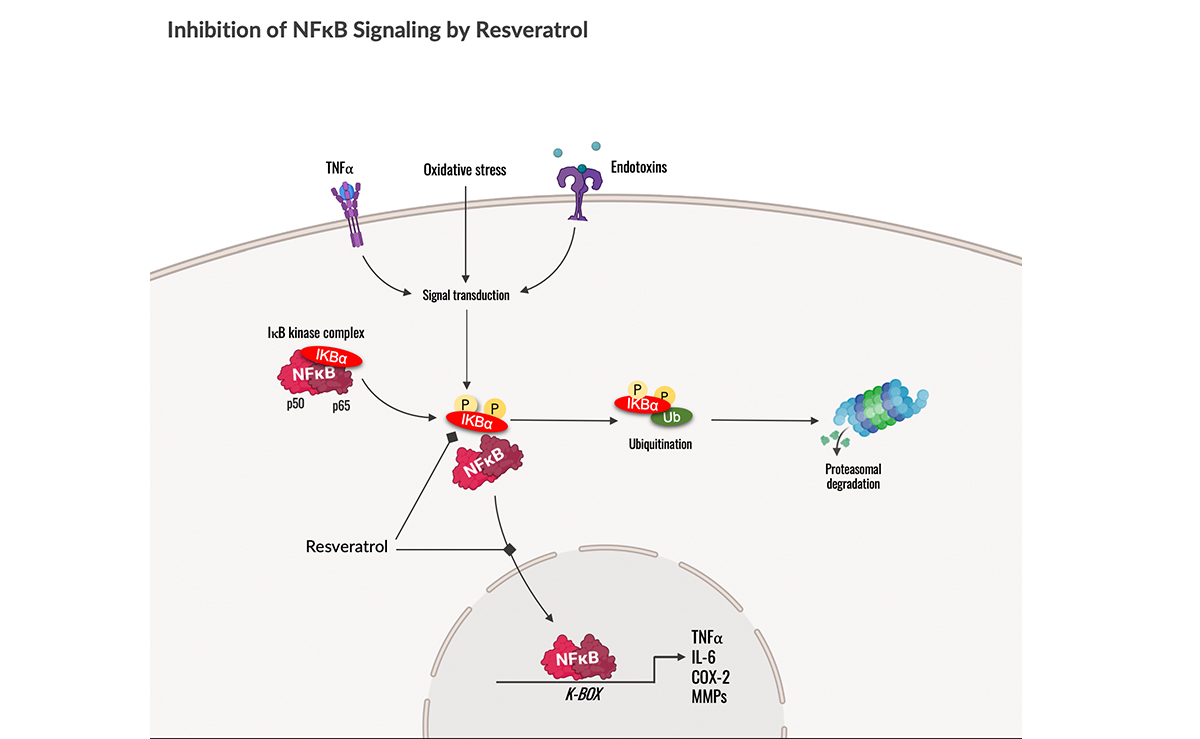
Figure 2; Resveratrol enhances cellular defenses against oxidative stress and inflammation by inhibiting nuclear factor kappa B (NFκB), a dimeric transcription factor that drives pro-inflammatory gene expression. Under basal circumstances, inactive NFκB is sequestered in the cytosol as part of the IκB kinase complex. Oxidative stress and immunological stimuli, such as pro-inflammatory cytokines (e.g., TNFα) and bacterial toxins, are perceived at the membrane via receptors that engage signal transduction and IκBα phosphorylation (yellow circles). Phosphorylated IκBα is then tagged with ubiquitin (Ub) for proteasomal degradation. This liberates NFκB to translocate to the nucleus, where it binds to DNA response elements (K-boxes) located in the promoters of target genes. DNA binding recruits the transcriptional machinery (not shown) and subsequent transcription of pro-inflammatory target genes, which include TNFα, interleukin (IL)-6, cyclooxygenase 2 (COX-2), and matrix metalloproteinases (MMPs). Resveratrol inhibits the phosphorylation of IκBα and nuclear translocation of NFκB. Image credit: Kelly Heim, Ph.D. Created with BioRender.com.
Like other phytonutrients, resveratrol protects the plant from pathogens, in particular fungi, and ultraviolet radiation.1 In preclinical experiments, resveratrol has also been shown to have immune-modulating properties, including modulation of both cellular and humoral immunity in the defence against pathogens.4
Clinical Uses
Alzheimer’s disease
Worldwide, it is estimated that 50 million people live with dementia, of which 60−70% have Alzheimer‘s disease (AD), the most common form of dementia.9 It is characterised by memory loss and cognitive impairment, and the main histopathological features of AD are amyloid-β (Aβ) plaques.10 Caloric restriction is thought to prevent or delay onset of AD, possibly through activation of SIRT1.11 As resveratrol also activates SIRT1, it has been studied in animal models of AD with promising results.12
One double-blind, placebo-controlled study of 104 patients with mild-to-moderate AD found statistically significant favourable effects on the biomarker Aβ40 in both blood and cerebrospinal fluid, but not on tau protein (another AD biomarker).13 The study was too small to detect significant clinical improvements. Interestingly, brain volume decreased more in patients on resveratrol than placebo, which the authors hypothesised may be due to reduced inflammation-related swelling. A retrospective follow-up study, using frozen samples from a subset of patients with AD confirmed by biomarkers at baseline (19 in the resveratrol and 19 in the placebo group), found significant changes in a number of cytokines and other biomarkers, suggesting resveratrol modulates neuro-inflammation and may improve the integrity of the blood−brain barrier.12 Clinical improvements were also seen in this subset of patients. The dose of resveratrol was increased gradually from 500 mg to 2000 mg per day, and the study duration was 1 year.
Another small randomised-controlled trial (RCT), looking at clinical outcomes, found that patients with AD on resveratrol deteriorated less than those on placebo over the course of the 1-year study, but this failed to reach statistical significance.10 This study used a much lower dose, 10 mg per day.
Clinical evidence for the use of resveratrol in AD is limited and, whilst some benefits on biomarkers have been observed, data on effects on clinical symptoms are too limited to reach a firm conclusion regarding the use of resveratrol in AD. It is important to bear in mind that AD is a very complex condition and that resveratrol may work best as part of a multi-faceted approach,14 although there is no evidence for this from clinical trials.
Autoimmune diseases
Autoimmune diseases are a leading cause of morbidity and mortality, and have been increasing over the past decades.15 Treatment options are often limited and associated with severe side-effects. The underlying cause of autoimmunity is an imbalanced immune system that has lost the ability to distinguish self from non-self, leading to local or systemic immune responses and inflammation.16 Whilst in vitro and animal studies have shown promise in a number of autoimmune diseases, human clinical trials are scarce.
One double-blind, placebo-controlled trial looked at resveratrol, 500 mg per day for 6 weeks, in patients with active mild to moderate ulcerative colitis (UC), and found significant improvements in disease activity, quality of life, oxidative stress and inflammatory markers compared with placebo.16,17 Another study in UC is currently ongoing.18
Another RCT compared resveratrol, 1000 mg per day for 3 months, alongside conventional treatment with conventional treatment alone in patients with rheumatoid arthritis (RA).19 Patients receiving resveratrol had a significant reduction in joint swelling and tenderness, disease activity score and inflammatory markers compared with those on standard treatment alone. Out of the 50 patients who received resveratrol, 41 showed a significant improvement, whilst nine were considered non-responders whose improvement in disease activity score did not reach statistical significance.
Whilst these two studies are promising for the use of resveratrol in patients with UC and RA, as well as potentially other autoimmune conditions, due to the scarcity of data it is difficult to make recommendations regarding dose or duration of supplementation.
Both RA and UC are associated with inflammation and increased oxidative stress, and the above studies suggest that the antioxidant and anti-inflammatory effects of resveratrol mediate its benefits at least in part. A small randomised pilot study in healthy volunteers also showed that resveratrol, 500 mg per day for 4 weeks, not only decreased anti-inflammatory markers and increased antioxidant status compared with controls, but also shifted the balance of T-cells (which are out of balance in autoimmunity) in a favourable way.20
Bone health
Osteoporosis is defined as low bone density (adjusted by age) and is an important risk factor for fractures, which can cause significant morbidity and mortality, especially in the elderly. In the USA, almost a quarter of women and over 5% of men over the age of 65 years have osteoporosis.21 As there are no symptoms until fractures occur, it is often called a ‘silent epidemic’. Resveratrol has shown promising results in preclinical research, and an emerging body of human clinical research corroborates such findings.22
A 2019 meta-analysis of six RCTs on bone biomarkers found that resveratrol significantly increased serum and bone alkaline phosphatase (biomarkers for bone formation).23 Except for one study in healthy elderly people, all trials were run in patients with metabolic syndrome (metS) or type 2 diabetes mellitus (T2DM). Dosages ranged from 150 mg to 1500 mg resveratrol per day for 4−24 weeks, with dosages of 1000 mg or above showing better results.
Another study in 193 patients with T2DM showed improvements in whole-body bone mineral density (BMD), bone mineral content and T-score (a measure of bone density relative to a 30-year-old person) after 6 months in those on 500 mg resveratrol per day.24 A study, involving 194 postmenopausal women, also found significant improvements of BMD in the lumbar spine and neck of the femur as well as a reduction in C-terminal telopeptide type-1 collagen levels (a bone resorption marker), but not in whole-body BMD, after 12 months of supplementation with resveratrol, 150 mg per day.22 In both studies, improvements were greater in those patients whose baseline status was worse.
In view of the wide range of dosages used in clinical trials, an optimal dose is uncertain and may to some extent depend on the patient population, for example, patients with T2DM or postmenopausal women.
A number of mechanisms are thought to play a role in the bone-protective effects of resveratrol. Resveratrol is thought to reduce the activity of osteoclasts (cells that break down bone) through its oestrogenic effects and possibly also through NF-ĸB-mediated pathways, whilst also inhibiting adipogenesis (formation of fat cells) to favour the formation of osteoblasts (the cells that build new bone) through SIRT1-related pathways.22,24
Cancer
By modulating various cancer-related pathways and gene expression, resveratrol exerts a number of anti-cancer effects, including inhibition of cancer cell growth and proliferation, induction of apoptosis (programmed cell death that is abnormal in cancerous cells), promotion of anti-tumour immune responses, and prevention of migration and invasion of cancer cells.4 Whilst preclinical research is promising, data from human trials are scarce.
One RCT in 112 men with prostate cancer, using pulverised muscadine grape skin, 500 mg or 4000 mg per day (providing 4 µg resveratrol per 500 mg) versus placebo for 4 months, found no overall effect of the supplement on doubling time of prostate-specific antigen (PSA; a prostate cancer marker).25 However, a subgroup of patients with a particular genetic polymorphism in the gene for SOD appeared to benefit with a reduction in PSA doubling time. Another study looked at the effect of resveratrol supplementation on hormone and PSA levels in men with metS, and found a lowering of testosterone precursors, but not PSA, testosterone, free testosterone and dihydrotestosterone.26 The dose used was 1000 mg resveratrol per day for 4 months. The authors therefore concluded that resveratrol was of no benefit in benign prostate hyperplasia (enlarged prostate, which is not thought to increase the risk of developing prostate cancer).
Three small pilot, pharmacokinetic and safety studies on resveratrol in colorectal cancer found improvements in some biomarkers: cleaved caspase-3 (a marker of apoptosis) in metastases,27 Wnt pathways (signal transduction pathways involved in carcinogenesis) in healthy but not cancerous colon cells,28 and reduced tumour cell proliferation.29 Dosages ranged from 80 mg to 5000 mg resveratrol per day for 8−21 days. Two studies observed no adverse events (AEs),28,29 whilst in the third several mild AEs were seen, mostly of a digestive nature.27
One RCT in 39 women at increased risk of breast cancer suggested a preventative effect of resveratrol, 5 mg or 50 mg per day for 12 weeks.30 There was no overall improvement in biomarkers in the resveratrol versus the placebo group. However, serum levels of resveratrol and its metabolites varied significantly between individuals, and there was an association between higher serum levels and decreased methylation of a cancer-related gene, RASSF-1a, which correlated with a decrease in prostaglandin E2, an inflammatory mediator that promotes cancer. These results, and those of the Paller et al. study in prostate cancer mentioned above,25 suggest that there are significant inter-individual differences in the response to resveratrol, possibly due to gene polymorphisms.
One small study with 24 patients with multiple myeloma was terminated early as five patients went into renal failure.31 The dose of resveratrol was 5000 mg per day. The authors state that this AE appears to be specific to patients with multiple myeloma, who are at particular risk, with renal impairment occurring in 50% of patients.
Overall, there is promising research in the field of cancer, but at present insufficient evidence to make any particular recommendations.
Heart disease and cardiovascular risk factors
Cardiovascular disease is a general term for diseases that affect the heart and blood vessels, and is the leading cause of death in the USA, being responsible for one in four deaths.32 Risk factors include hypertension, abnormal blood lipids, smoking and poor diet. Inflammation and oxidative stress play important roles in the development of CVD, so the antioxidant and anti-inflammatory effects of resveratrol should be of benefit in the prevention and/or management of CVD. As mentioned above, attention to the potential cardioprotective effects of resveratrol came through the observation of the ‘French paradox’, the low rates of heart disease in areas with high consumption of red wine, a rich dietary source of resveratrol.2
More than 20 clinical studies have evaluated the effectiveness of resveratrol on a number of cardiovascular risk factors, with inconsistent results. A recent meta-analysis of 17 studies involving 651 subjects found statistically significant benefits of resveratrol in improving the homeostatic model assessment for insulin resistance (HOMA-IR), LDL- and total cholesterol, but not any other cardiometabolic biomarkers, including blood pressure and other blood lipids and markers of glycaemic control.33
A meta-analysis of 17 studies evaluating hypertension found no overall benefit of resveratrol, but a subgroup of patients with diabetes receiving dosages over 300 mg per day showed a significant reduction in blood pressure.34 Another meta-analysis of 20 studies focussed on blood lipids and found no benefit of resveratrol.35 Similarly, a 2015 meta-analysis of 10 studies found no effect on C-reactive protein (CRP; a marker of inflammation), blood lipids, glucose or blood pressure.36
Looking at the individual studies used in the meta-analyses shows that there is significant inconsistency between trial outcomes, with some showing benefits, some nil effects and some even a worsening.35,37
A few more recent trials, not included in the above meta-analyses, on the whole showed promising results, with improvements in clinical features in patients with heart failure,38 glycaemic control and high-density lipoprotein (HDL) cholesterol in patients with T2DM,39,40 oxidative stress and antioxidant status in patients with T2DM,39 atherosclerosis biomarkers in patients with T2DM,40 and echocardiography and 24-h electrocardiogram outcomes in patients with coronary heart disease.40 Studies used between 100 mg and 1000 mg resveratrol per day for 1−3 months.
One study found a non-significant improvement in a number of biomarkers with 300 mg resveratrol per day, but a worsening with 1000 mg per day over 3 months.6
The reasons for these contradictory results are unclear and appear to be unrelated to dosage. Dosages used in clinical trials have varied widely, from 10 mg per day to 1000 mg per day, and durations from 14 days to 1 year.
Overall, there appears to be a benefit of resveratrol in improving CVD risk factors, although evidence from clinical trials remains inconclusive with regards to dosages and duration as well as which populations may benefit most and for which risk factors.
Cognitive function
In animal experiments, resveratrol has been found to be neuroprotective, and to improve cognition and brain function.41
However, two recent reviews and meta-analyses of nine and 11 human RCTs, respectively, have only found small improvements that were not statistically significant, except for one outcome measure, delayed recognition, for which there was a statistically significant improvement.41,42 Looking at the studies individually, five found some benefits in terms of improved memory and psychomotor speed. Different assessments and outcome measures were used across the studies. Dosages ranged from 75 mg to 1000 mg resveratrol per day or grape powder/juice, whilst duration ranged from 2 weeks to 6 months, and two studies evaluated acute effects in 1-day trials. There did not appear to be a connection between dose or duration of treatment and results.
In 2020, the results of a 24-month double-blind, placebo-controlled crossover trial were published.43,44 One-hundred and twenty-nine postmenopausal women took either 75 mg resveratrol or placebo twice a day for 12 months, and then crossed over to the other treatment. A statistically significant 33% improvement in overall cognitive function was observed, with women over 65 years benefitting more in verbal memory, a decline of which can be an early sign of AD. Significant improvements were also seen in cerebrovascular function and insulin sensitivity, and no apparent side-effects were noted. The authors of this study conclude that the benefits may be partly mediated through endothelium-dependent cerebrovascular function, which declines with oestrogen deficiency and age. Resveratrol may act through various pathways including SIRT1 and oestrogen receptors to increase endothelial nitric oxide.44
Although results from clinical trials are mixed, longer-term supplementation of 12 months, with relatively low-dose resveratrol, for example 150 mg per day, may provide benefits in terms of cognitive and cerebrovascular function.
Diabetes and metabolic syndrome
There has been a significant increase in T2DM over the past decades, and it was estimated that in 2018, 13% of all US adults had diabetes, 90−95% of these having T2DM, and over a fifth not being aware that they had the disease. Based on measurements of glycosylated haemoglobin (HbA1c; a longer-term measure of glycaemic control), it was estimated that a further third of all US adults were prediabetic.45,46 Diabetes significantly increases the risk of CVD and can also lead to a number of complications, including kidney disease, eye-related problems, neuropathy and leg ulcers.
Metabolic syndrome (metS) is not a disease as such but a cluster of cardiovascular risk factors and is closely related to T2DM. It is defined as having at least three out of the five following markers: elevated waist circumference (WC); elevated triglycerides; low HDL-cholesterol; elevated blood pressure; and elevated fasting glucose.47
Oxidative stress and inflammation play important roles in both the development of T2DM as well as its complications, therefore reducing oxidative stress and inflammation can be beneficial.
There are over 30 human clinical trials looking at resveratrol in T2DM or metS and related disorders (which would include T2DM), with inconsistent results.
Four meta-analyses looked specifically at T2DM. One meta-analysis found that resveratrol improved fasting glucose and insulin, HOMA-IR and blood pressure, but not HbA1c, LDL- and HDL-cholesterol.48 Another meta-analysis in T2DM found that resveratrol improved triglyceride levels, but also led to an increase in LDL- and total cholesterol in some patient groups.49 One meta-analysis looked specifically at levels of CRP (a marker of inflammation) in type 2 diabetics and found benefits after at least 12 weeks of resveratrol supplementation.50 A Cochrane review and meta-analysis in 2020 came to the conclusion that: “The limited available research does not provide sufficient evidence to support any effect, beneficial or adverse, of 4−5 weeks of 10 mg to 1000 mg of resveratrol in adults with T2DM”.51 However, this review only included three studies, compared with six−10 RCTs included in the other meta-analyses.
Benefits of resveratrol in T2DM have been reported with regards to improved bone health with 500 mg per day for 6 months,24 and healing of diabetic ulcers with 100 mg per day for 60 days.52 Acute supplementation of a single dose of 75 mg resveratrol has been shown to improve cerebrovascular function, neurovascular coupling (the neuronal regulation of blood flow to the brain) and cognitive function in patients with T2DM, although longer-term studies in this area are lacking.53,54
Only one small pilot study looked into benefits for type 1 diabetes mellitus (T1DM).55 In this open, uncontrolled trial, 13 patients with T1DM received 1000 mg resveratrol for 8 weeks. Significant improvements in fasting glucose and HbA1c, but not other markers of glycaemic control, kidney or liver function, were seen. There was also a significant improvement in markers of oxidative stress but not inflammation.
More reviews and meta-analyses looked into the effects of resveratrol in patients with metS and related disorders, which include T2DM. A 2021 meta-analysis of 30 studies, involving 1651 participants, found significant improvements in glucose and insulin, whilst results for HOMA-IR failed to reach statistical significance.56 Significant improvements in HbA1c were seen only with supplementation for more than 3 months in this meta-analysis, which would be expected in view of the fact that HbA1c reflects glycaemic control over the previous 2−3 months. Subgroup analysis showed that these improvements were limited to patients with T2DM.
A meta-analysis of 31 studies, with 1722 participants, looked at blood lipids and liver enzymes in patients with metS and related disorders.57 Whilst there was a significant decrease in total cholesterol, there were no changes in LDL- or HDL-cholesterol and, whilst two out of three liver enzymes remained unchanged, one actually increased. A meta-analysis of 10 studies involving 296 patients with metS found significant favourable effects on glucose and WC with more than 500 mg resveratrol per day taken for longer than 10 weeks, but no effect on blood lipids or weight.58 Another meta-analysis looked at blood pressure (28 studies, 1748 subjects) and endothelial function (six studies only), and found no changes in blood pressure but significant improvements in endothelial function.59 A meta-analysis of 24 studies (1112 patients) looking at oxidative stress and inflammatory markers in patients with metS and related disorders found significant decreases in CRP and TNF-α, but not SOD or IL-6.60
Overall, whilst not all individual studies report benefits, the results are promising for the use of resveratrol in T2DM and metS. Dosages in the clinical trials ranged from 8 mg to 3000 mg per day, for durations of 1 week to 1 year. Whilst longer duration appears to be more beneficial, the heterogeneity of the results does not allow at this point to suggest a dose.
The reason for the differing results is unclear and may be due to so far unknown genetic factors. One study looked at a single-nucleotide polymorphism (SNP; a genetic variation of one gene) for SIRT1 in diabetics and found that, whilst the SNP resulted in a lowered level of SIRT1 expression following resveratrol supplementation, it did not have any significant effect on any biochemical markers.61
One small double-blind pilot study of 28 obese men with metS found that resveratrol, 2000 mg per day for 30 days, led to a significant improvement in insulin sensitivity and glucose homeostasis in Caucasians, whereas no effects were seen in non-Caucasians, an observation that was not explained by plasma levels of resveratrol or its metabolites.62 This study also evaluated changes in the microbiome and found that resveratrol led to a significant change in microbiome balance that differed between Caucasians and non-Caucasians, with the former having an increase in Akkermansia muciniphila, a bacterium that has been associated with a lower risk of obesity, diabetes and low-grade inflammation.62 These results suggest that the microbiome composition and/or racial background may affect whether or not resveratrol exerts benefits in the individual.
The antioxidant and anti-inflammatory effects of resveratrol are thought to mediate its potential benefits in T2DM.50 Improvements in insulin signalling (through a signalling pathway called Akt) have been observed.63 Another study found that resveratrol upregulated SIRT1 and AMP-activated protein kinase (AMPK), an enzyme that improves insulin sensitivity by upregulating glucose transporter type 4 (GLUT4; which transports glucose into cells (see figure 3). This study also observed that whilst activity levels went down in the resveratrol group, their energy expenditure/basal metabolic rate went up, compared with the placebo group, although there were no differences in markers of glycaemic control, suggesting that resveratrol may have an exercise-mimetic effect in patients with T2DM. Finally, the study by Walker et al. looking at the microbiome, mentioned above, suggests that resveratrol may exert beneficial effects through affecting favourable changes of the microbiome.62
Figure 3: Resveratrol enhances insulin-mediated glucose disposal via the AMPK/SIRT1 Axis
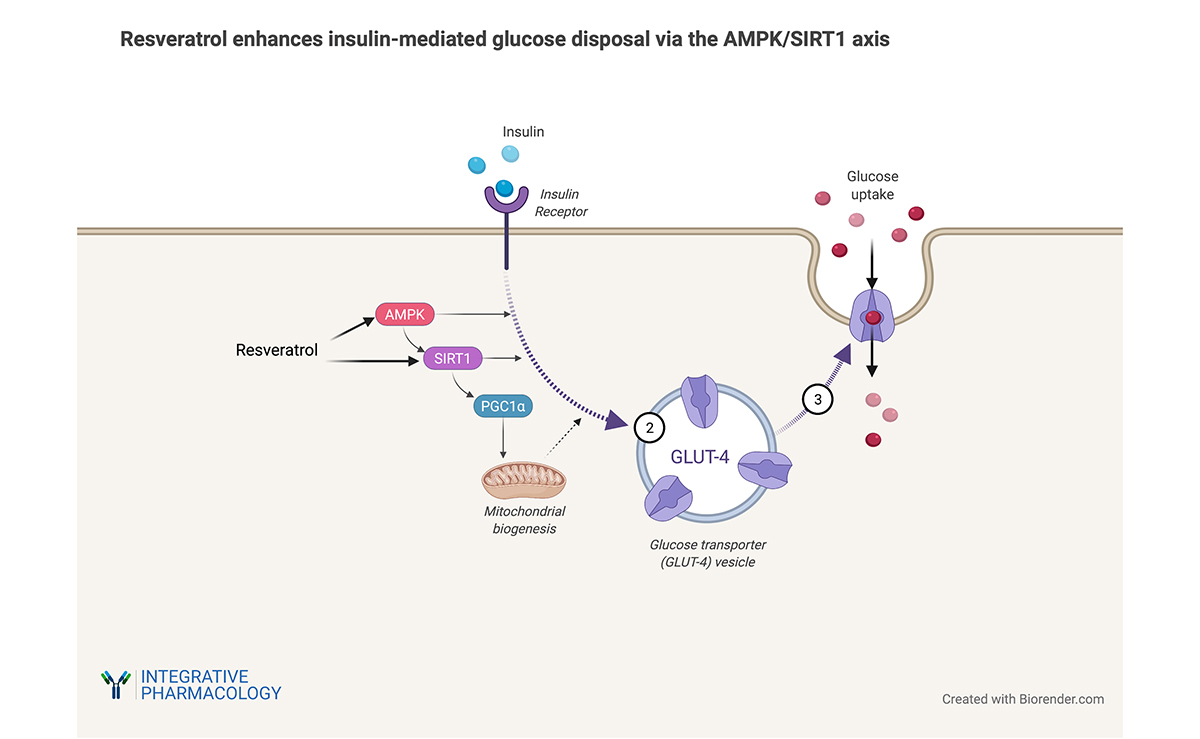
Figure 3; Resveratrol enhances insulin-stimulated glucose transporter (GLUT4) localization to the cell membrane by activating AMP kinase (AMPK), sirtuin 1 (SIRT1) and PPAR-gamma coactivator 1 alpha (PGC-1α). This pathway induces mitochondrial biogenesis, which improves in insulin sensitivity in skeletal muscle. Image credit: Kelly Heim, Ph.D. Created with BioRender.com.
Non-alcoholic fatty liver disease
Non-alcoholic fatty liver disease (NAFLD) is characterised by a build-up of fat within liver cells, and risk factors include obesity/overweight, metS and T2DM. NAFLD is the most common liver disease in the USA, affecting an estimated 24% of adults, and 1.5−6.5% of adults are thought to have non-alcoholic steatohepatitis (NASH).65 The equivalent numbers in the UK are 20−30% for NAFLD and 2−3% for NASH.66
A number of clinical trials have evaluated the potential benefits of resveratrol in NAFLD. A meta-analysis including six studies and 266 patients with NAFLD found significant decreases in the inflammatory markers TNF-α and high-sensitivity CRP (hsCRP), but no significant changes in blood lipids, anthropometric data, glycaemic control or liver function tests.67 Another meta-analysis that looked only at the two liver enzymes alanine transaminase (ALT) and aspartate aminotransferase (AST), involving five studies and 216 patients, found benefits in specific subgroups, people under the age of 45 years and those who are not obese.68 This study also found favourable effects with dosages under 1000 mg resveratrol per day for longer than 12 weeks. In both meta-analyses, dosages used ranged between 300 mg and 3000 mg resveratrol per day for 8−24 weeks.
Looking at the individual studies, it appears that those using a daily dose of 300 mg or 500 mg for 3 months found more benefits, in particular with regards to ALT and inflammatory markers,69,70 than those using higher dosages, where there were no consistent improvements.8,71,72,73
Overall, the evidence suggests that lower dosages of resveratrol (300−500 mg per day) may be of benefit for patients with NAFLD with regards to reducing inflammation and the liver enzyme ALT, although other biomarkers, including those for glycaemic control, blood lipids and anthropometric measures, do not appear to respond to resveratrol supplementation in this patient group.
Proposed mechanisms by which resveratrol may ameliorate NAFLD are its ability to upregulate SIRT1, which has been shown to increase insulin sensitivity and decrease inflammation, and AMPK, which is thought to have a positive effect on lipid metabolism.64
Obesity
Obesity is an important risk factor for a number of conditions, including CVD, T2DM and some cancers, and as such is a major public health issue.74 In 2017−2018, the prevalence of obesity, defined as a body mass index (BMI) of 30 kg m−2 and over, in adults in the USA was 42.4%, and 9.2% were severely obese (BMI > 40 kg m−2).75 Obesity is associated with chronic low-grade inflammation, and adipose (fat) tissue secretes adipokines, compounds such as adiponectin and leptin, which are involved in the regulation of many metabolic processes as well as eating behaviour.76 Resveratrol has been studied for metabolic health in overweight and obese patients.
A 2021 meta-analysis of 19 studies showed no benefit of resveratrol on weight or BMI, but a small decrease in WC.77 Looking at the individual studies, only three of them showed benefits either on their own or together with the weight loss drug Orlistat. A 2019 meta-analysis of 28 trials found statistically significant reductions in BMI, weight and WC, although effect sizes were small, −0.17 kg m−2, −0.51 kg and 0.79 cm, respectively.78 Yet another meta-analysis of 36 studies also found statistically significant reductions in weight, BMI and WC, but effect sizes were even smaller.79 Across all the studies, resveratrol dose ranged from 8 mg to 3000 mg per day, for 1 week to 1 year. Smaller dosages (less than 200 mg79 or 500 mg78) appeared to be more effective, duration had to be at least 12 weeks to see effects, and people with obesity and/or T2DM were more likely to see benefits.78,79
Whilst one of the above meta-analyses found no effect of resveratrol on adiponectin or leptin,79 another meta-analysis looking specifically at adipokines found a statistically significant effect on adiponectin but not leptin.76
Whilst results from clinical trials are mixed, resveratrol does not appear to have a clinically significant effect on weight loss.
As for possible mechanisms for resveratrol in weight loss, one study found that resveratrol may increase basic metabolic rate/energy expenditure.64 This has also been observed in animal studies.79 One small study looked at the effect of resveratrol on growth hormones (GHs) in obese men, but found no effect on circulating levels of insulin-like growth hormone-1 (IGH-1) or GH signalling in human muscle and fat cells.80 Another small mechanistic study looked at adipose tissue morphology and gene expression in obese men, and saw a significantly decreased size of fat cells and an upregulation of various genes, including some involved in cellular lipid metabolism.81
Safety
A 2014 review on metabolic, biological and potential toxic effects of resveratrol reported in clinical trials concluded that resveratrol is generally well tolerated, and that with a daily dose of 500 mg or with durations of less than 1 month no AEs have been observed.82 With higher dosages some AEs were reported, which were generally mild and transient, and most commonly affected the digestive system, including diarrhoea, abdominal pain, nausea and flatulence. At a very high dose (5000 mg per day for 2 weeks), chills, lethargy, rash, skin irritation and vascular flushing have been observed, in addition to gastrointestinal side-effects, in patients with metastatic colorectal cancer.27 In patients undergoing peritoneal dialysis, receiving either 150 mg or 450 mg resveratrol per day for 12 weeks, constipation, headache, muscle cramps, fatigue and memory loss have been reported, which led to discontinuation of resveratrol in four patients, although the authors did not state whether they considered these AEs as related to resveratrol or which dose they appeared with.83
One serious AE of fever and low white blood cell count occurred in a patient with NAFLD after taking 1500 mg per day for 10 days and recurred on rechallenge.71 As mentioned above under cancer, five cases of kidney failure have been seen in patients with multiple myeloma following the use of resveratrol, 5000 mg per day, but this serious side-effect is thought to be specific to this patient population.31
Shaito et al. discuss possible harmful effects in their 2020 review, and suggest that resveratrol may have a biphasic effect on cellular redox status (the balance between pro-and antioxidants), exerting antioxidant effects at low and pro-oxidant effects with high dosages, at least in in vitro and animal experiments.84 This has in fact been observed in some studies, where low dosages had better outcomes than higher ones, and can be explained with the concept of hormesis, where a beneficial effect is caused by exposure to low doses of an agent known to be toxic at higher doses.
Drug and Disease Interactions
At a dose of 1000 mg per day or more, resveratrol was reported to inhibit some cytochrome P450 isoenzymes, including CYP3A4, CYP2C9 and CYP2D6, while activating CYP1A, which may lead to interactions with many drugs that are metabolised through these enzymes.84,85
Resveratrol is thought to have anti-platelet effects, and should therefore be used with caution in people with bleeding disorders or on blood-thinning medication.85
Pregnancy, Breastfeeding and Children
Resveratrol is considered to be safe in children, and pregnant and breastfeeding women in amounts typically found in foods.85 There are no clinical trials investigating oral supplementation with resveratrol in these populations.
Conclusions
At present, the evidence base for the use of resveratrol in clinical practice is limited, and more research is needed to inform the choice of doses and patient populations that may benefit most. Human clinical research suggests good potential for resveratrol for bone health, limited but promising evidence for its use in AD, autoimmune disease (UC, RA) and cancer prevention (breast, colorectal). Evidence is mixed/contradictory, but overall promising for CVD, cognitive function, NAFLD and T2DM/metS. Generally, resveratrol is considered well tolerated and safe for clinical use.
Acknowledgements
Author contributions: K. Elgar carried out the literature review and formulated the manuscript.
Peer-reviewers and editors: the Nutritional Medicine Institute thanks the peer-reviewers and editors for their important contributions.
Funding: Open Access publication was supported by an unrestricted donation from Pure Encapsulations, Sudbury, MA, USA. No other funding or sponsorship has been received for this work.
Declaration of interest: K. Elgar has received consultancy fees from Pure Encapsulations, Sudbury, MA, USA. This article is the independent work of the author and Pure Encapsulations was not involved in the decision to publish this research.
References
1 Riccio, B. V. F., Spósito, L., Carvalho, G. C., Ferrari, P. C. & Chorilli, M. (2020) Resveratrol isoforms and conjugates: A review from biosynthesis in plants to elimination from the human body. Arch. Pharm. (Weinheim), 353, e2000146.
2 Berman, A. Y., Motechin, R. A., Wiesenfeld, M. Y. & Holz, M. K. (2017) The therapeutic potential of resveratrol: a review of clinical trials. NPJ Precis. Oncol., 1, 35.
3 Jang, M. et al. (1997) Cancer chemopreventive activity of resveratrol, a natural product derived from grapes. Science, 275, 218–220.
4 Meng, X., Zhou, J., Zhao, C.-N., Gan, R.-Y. & Li, H.-B. (2020) Health benefits and molecular mechanisms of resveratrol: A narrative review. Foods (Basel, Switzerland), 9, 340.
5 Rauf, A. et al. (2017) A comprehensive review of the health perspectives of resveratrol. Food Funct., 8, 4284–4305.
6 Mankowski, R. T. et al. (2020) Higher dose of resveratrol elevated cardiovascular disease risk biomarker levels in overweight older adults − a pilot study. Exp. Gerontol., 131, 110 821.
7 Mansur, A. P. et al. (2017) Serum concentrations and gene expression of sirtuin 1 in healthy and slightly overweight subjects after caloric restriction or resveratrol supplementation: A randomized trial. Int. J. Cardiol., 227, 788–794.
8 Asghari, S., Asghari-Jafarabadi, M., Somi, M.-H., Ghavami, S.-M. & Rafraf, M. (2018) Comparison of calorie-restricted diet and resveratrol supplementation on anthropometric indices, metabolic parameters, and serum sirtuin-1 levels in patients with nonalcoholic fatty liver disease: A randomized controlled clinical trial. J. Am. Coll. Nutr., 37, 223–233.
9 World Health Organization (2020) Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia.
10 Zhu, C. W. et al. (2018) A randomized, double-blind, placebo-controlled trial of resveratrol with glucose and malate (RGM) to slow the progression of Alzheimer’s disease: A pilot study. Alzheimer’s Dement. (New York, NY), 4, 609–616.
11 Van Cauwenberghe, C., Vandendriessche, C., Libert, C. & Vandenbroucke, R. E. (2016) Caloric restriction: Beneficial effects on brain aging and Alzheimer’s disease. Mamm. Genome, 27, 300–319.
12 Moussa, C. et al. (2017) Resveratrol regulates neuro-inflammation and induces adaptive immunity in Alzheimer’s disease. J. Neuroinflammation, 14, 1.
13 Turner, R. S. et al. (2015) A randomized, double-blind, placebo-controlled trial of resveratrol for Alzheimer disease. Neurology, 85, 1383–1391.
14 Kurakin, A. & Bredesen, D. E. (2020) Alzheimer’s disease as a systems network disorder: chronic stress/dyshomeostasis, innate immunity, and genetics. Aging (Albany. NY), 12, 17 815–17 844.
15 Lerner, A., Jeremias, P. & Matthias, T. (2015) The world incidence and prevalence of autoimmune diseases is increasing. Int. J. Celiac Dis., 3, 151–155.
16 Oliveira, A. L. de B. et al. (2017) Resveratrol role in autoimmune disease−a mini-review. Nutrients, 9, 1306.
17 Samsamikor, M., Daryani, N. E., Asl, P. R. & Hekmatdoost, A. (2016) Resveratrol supplementation and oxidative/anti-oxidative status in patients with ulcerative colitis: A randomized, double-blind, placebo-controlled pilot study. Arch. Med. Res., 47, 304–309.
18 Chen, Y.-H. & Xiang, Y. (2019) Efficacy of resveratrol for the treatment in patients with ulcerative colitis: Study protocol. Medicine (Baltimore), 98, e17938.
19 Khojah, H. M., Ahmed, S., Abdel-Rahman, M. S. & Elhakeim, E. H. (2018) Resveratrol as an effective adjuvant therapy in the management of rheumatoid arthritis: A clinical study. Clin. Rheumatol., 37, 2035–2042.
20 Espinoza, J. L. et al. (2017) The repeated administration of resveratrol has measurable effects on circulating T-cell subsets in humans. Oxid. Med. Cell. Longev., 2017, 6781872.
21 Looker, A. C. & Frank, S. M. (2015) Percentage of adults aged 65 and over with osteoporosis or low bone mass at the femur neck or lumbar spine: United States, 2005–2010. National Center for Health Statistics https://www.cdc.gov/nchs/data/hestat/osteoporsis/osteoporosis2005_2010.htm.
22 Wong, R. H., Thaung Zaw, J. J., Xian, C. J. & Howe, P. R. (2020) Regular supplementation with resveratrol improves bone mineral density in postmenopausal women: A randomized, placebo-controlled trial. J. Bone Miner. Res., 35, 2121–2131.
23 Asis, M. et al. (2019) Effects of resveratrol supplementation on bone biomarkers: A systematic review and meta-analysis. Ann. N. Y. Acad. Sci., 1457, 92–103.
24 Bo, S. et al. (2018) Effects of resveratrol on bone health in type 2 diabetic patients. A double-blind randomized-controlled trial. Nutr. Diabetes, 8, 51.
25 Paller, C. J. et al. (2018) Muscadine grape skin extract (MPX) in men with biochemically recurrent prostate cancer: A randomized, multicenter, placebo-controlled clinical trial. Clin. Cancer Res., 24, 306–315.
26 Kjaer, T. N. et al. (2015) Resveratrol reduces the levels of circulating androgen precursors but has no effect on, testosterone, dihydrotestosterone, PSA levels or prostate volume. A 4-month randomised trial in middle-aged men. Prostate, 75, 1255–1263.
27 Howells, L. M. et al. (2011) Phase I randomized, double-blind pilot study of micronized resveratrol (SRT501) in patients with hepatic metastases−safety, pharmacokinetics, and pharmacodynamics. Cancer Prev. Res. (Phila.), 4, 1419–1425.
28 Nguyen, A. V et al. (2009) Results of a phase I pilot clinical trial examining the effect of plant-derived resveratrol and grape powder on Wnt pathway target gene expression in colonic mucosa and colon cancer. Cancer Manag. Res., 1, 25–37.
29 Patel, K. R. et al. (2010) Clinical pharmacology of resveratrol and its metabolites in colorectal cancer patients. Cancer Res., 70, 7392–7399.
30 Zhu, W. et al. (2012) Trans-resveratrol alters mammary promoter hypermethylation in women at increased risk for breast cancer. Nutr. Cancer, 64, 393–400.
31 Popat, R. et al. (2013) A phase 2 study of SRT501 (resveratrol) with bortezomib for patients with relapsed and or refractory multiple myeloma. Br. J. Haematol.,160, 714–717.
32 Centres for Disease Control and Prevention (2020) Heart Disease Statistics and Maps. https://www.cdc.gov/heartdisease/facts.htm.
33 Sergi, C., Chiu, B., Feulefack, J., Shen, F. & Chiu, B. (2020) Usefulness of resveratrol supplementation in decreasing cardiometabolic risk factors comparing subjects with metabolic syndrome and healthy subjects with or without obesity: Meta-analysis using multinational, randomised, controlled trials. Arch. Med. Sci. Atheroscler. Dis., 5, e98–e111.
34 Fogacci, F. et al. (2019) Effect of resveratrol on blood pressure: A systematic review and meta-analysis of randomized, controlled, clinical trials. Crit. Rev. Food Sci. Nutr., 59, 1605–1618.
35 Haghighatdoost, F. & Hariri, M. (2018) Effect of resveratrol on lipid profile: An updated systematic review and meta-analysis on randomized clinical trials. Pharmacol. Res., 129, 141–150.
36 Sahebkar, A. et al. (2015) Lack of efficacy of resveratrol on C-reactive protein and selected cardiovascular risk factors−Results from a systematic review and meta-analysis of randomized controlled trials. Int. J. Cardiol., 189, 47–55.
37 Dyck, G. J. B., Raj, P., Zieroth, S., Dyck, J. R. B. & Ezekowitz, J. A. (2019) The effects of resveratrol in patients with cardiovascular disease and heart failure: A narrative review. Int. J. Mol. Sci., 20, 904.
38 Gal, R. et al. (2020) Hemorheological alterations in patients with heart failure with reduced ejection fraction treated by resveratrol. Cardiovasc. Ther., 2020, 7262474.
39 Hoseini, A. et al. (2019) The effects of resveratrol on metabolic status in patients with type 2 diabetes mellitus and coronary heart disease. Food Funct., 10, 6042–6051.
40 Abdollahi, S. et al. (2019) The effect of resveratrol supplementation on cardio-metabolic risk factors in patients with type 2 diabetes: A randomized, double-blind controlled trial. Phytother. Res., 33, 3153–3162.
41 Khorshidi, F. et al. (2021) Resveratrol: A ‘miracle’ drug in neuropsychiatry or a cognitive enhancer for mice only? A systematic review and meta-analysis. Ageing Res. Rev., 65, 101 199.
42 Marx, W. et al. (2018) Effect of resveratrol supplementation on cognitive performance and mood in adults: A systematic literature review and meta-analysis of randomized controlled trials. Nutr. Rev., 76, 432–443.
43 Thaung Zaw, J. J., Howe, P. R. & Wong, R. H. (2020) Long-term effects of resveratrol on cognition, cerebrovascular function and cardio-metabolic markers in postmenopausal women: A 24-month randomised, double-blind, placebo-controlled, crossover study. Clin. Nutr., doi:10.1016/j.clnu.2020.08.025.
44 Thaung Zaw, J. J., Howe, P. R. C. & Wong, R. H. X. (2020) Sustained cerebrovascular and cognitive benefits of resveratrol in postmenopausal women. Nutrients, 12, 828.
45 Centres for Disease Control and Prevention (2019) Type 2 Diabetes. https://www.cdc.gov/diabetes/basics/type2.html.
46 Centres for Disease Control and Prevention (2020) National Diabetes Statistics Report, 2020. https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf.
47 Alberti, K. G. M. M. et al. (2009) Harmonizing the metabolic syndrome. Circulation, 120, 1640–1645.
48 Zhu, X., Wu, C., Qiu, S., Yuan, X. & Li, L. (2017) Effects of resveratrol on glucose control and insulin sensitivity in subjects with type 2 diabetes: Systematic review and meta-analysis. Nutr. Metab. (Lond.), 14, 60.
49 Zhao, H. et al. (2019) Effect of resveratrol on blood lipid levels in patients with type 2 diabetes: A systematic review and meta-analysis. Obesity (Silver Spring), 27, 94–102.
50 Hosseini, H. et al. (2020) The effect of resveratrol supplementation on C-reactive protein (CRP) in type 2 diabetic patients: Results from a systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med., 49, 102 251.
51 Jeyaraman, M. M. et al. (2020) Resveratrol for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev., 1, CD011919.
52 Bashmakov, Y. K. et al. (2014) Resveratrol promotes foot ulcer size reduction in type 2 diabetes patients. ISRN Endocrinol., 2014, 816 307.
53 Wong, R. H. X., Raederstorff, D. & Howe, P. R. C. (2016) Acute resveratrol consumption improves neurovascular coupling capacity in adults with type 2 diabetes mellitus. Nutrients, 8, 425.
54 Wong, R. H. X., Nealon, R. S., Scholey, A. & Howe, P. R. C. (2016) Low dose resveratrol improves cerebrovascular function in type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis., 26, 393–399.
55 Movahed, A. et al. (2020) Efficacy and safety of resveratrol in type 1 diabetes patients: A two-month preliminary exploratory trial. Nutrients, 12, 161.
56 García-Martínez, B. I., Ruiz-Ramos, M., Pedraza-Chaverri, J., Santiago-Osorio, E. & Mendoza-Núñez, V. M. (2021) Hypoglycemic effect of resveratrol: A systematic review and meta-analysis. Antioxidants (Basel, Switzerland), 10, 69.
57 Akbari, M. et al. (2020) The effects of resveratrol on lipid profiles and liver enzymes in patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Lipids Health Dis., 19, 25.
58 Asgary, S., Karimi, R., Momtaz, S., Naseri, R. & Farzaei, M. H. (2019) Effect of resveratrol on metabolic syndrome components: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord., 20, 173–186.
59 Akbari, M. et al. (2019) The effects of resveratrol supplementation on endothelial function and blood pressures among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. High Blood Press. Cardiovasc. Prev., 26, 305–319.
60 Tabrizi, R. et al. (2018) The effects of resveratrol supplementation on biomarkers of inflammation and oxidative stress among patients with metabolic syndrome and related disorders: A systematic review and meta-analysis of randomized controlled trials. Food Funct., 9, 6116–6128.
61 Gambino, R. et al. (2019) Rs12778366 single nucleotide polymorphism of Sirtuin 1 (SIRT1) and response to resveratrol supplementation in patients with type 2 diabetes mellitus. Acta Diabetol., 56, 963–966.
62 Walker, J. M. et al. (2019) The effects of trans-resveratrol on insulin resistance, inflammation, and microbiota in men with the metabolic syndrome: A pilot randomized, placebo-controlled clinical trial. J. Clin. Transl. Res., 4, 122–135.
63 Brasnyó, P. et al. (2011) Resveratrol improves insulin sensitivity, reduces oxidative stress and activates the Akt pathway in type 2 diabetic patients. Br. J. Nutr., 106, 383–389.
64 Goh, K. P. et al. (2014) Effects of resveratrol in patients with type 2 diabetes mellitus on skeletal muscle SIRT1 expression and energy expenditure. Int. J. Sport Nutr. Exerc. Metab., 24, 2–13.
65 NIH (2021) Definition & Facts of NAFLD & NASH. https://www.niddk.nih.gov/health-information/liver-disease/nafld-nash/definition-facts.
66 National Insitute for Health and Care Excellence (NICE) (2016) Non-alcoholic fatty liver disease (NAFLD): Assessment and management. NIC Guideline, https://www.nice.org.uk/guidance/ng49.
67 Rafiee, S. et al. (2021) Efficacy of resveratrol supplementation in patients with nonalcoholic fatty liver disease: A systematic review and meta-analysis of clinical trials. Complement. Ther. Clin. Pract., 42, 101 281.
68 Wei, S. & Yu, X. (2020) Efficacy of resveratrol supplementation on liver enzymes in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Complement. Ther. Med., 57, 102 635.
69 Faghihzadeh, F., Adibi, P., Rafiei, R. & Hekmatdoost, A. (2014) Resveratrol supplementation improves inflammatory biomarkers in patients with nonalcoholic fatty liver disease. Nutr. Res., 34, 837–843.
70 Chen, S. et al. (2015) Resveratrol improves insulin resistance, glucose and lipid metabolism in patients with non-alcoholic fatty liver disease: A randomized controlled trial. Dig. Liver Dis., 47, 226–232.
71 Heebøll, S. et al. (2016) Placebo-controlled, randomised clinical trial: High-dose resveratrol treatment for non-alcoholic fatty liver disease. Scand. J. Gastroenterol., 51, 456–464.
72 Chachay, V. S. et al. (2014) Resveratrol does not benefit patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol., 12, 2092−2103.e6.
73 Farzin, L., Asghari, S., Rafraf, M., Asghari-Jafarabadi, M. & Shirmohammadi, M. (2020) No beneficial effects of resveratrol supplementation on atherogenic risk factors in patients with nonalcoholic fatty liver disease. Int. J. Vitam. Nutr. Res., 90, 279–289.
74 Christenson, J. et al. (2016) The effects of resveratrol supplementation in overweight and obese humans: A systematic review of randomized trials. Metab. Syndr. Relat. Disord., 14, 323–333.
75 Hales, C., Carroll, M., Fryar, C. & Ogden, C. (2020) Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief, no 360. https://www.cdc.gov/nchs/products/databriefs/db360.htm.
76 Mohammadi-Sartang, M., Mazloom, Z., Sohrabi, Z., Sherafatmanesh, S. & Barati-Boldaji, R. (2017) Resveratrol supplementation and plasma adipokines concentrations? A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res., 117, 394–405.
77 Delpino, F. M., Figueiredo, L. M., Caputo, E. L., Mintem, G. C. & Gigante, D. P. (2021) What is the effect of resveratrol on obesity? A systematic review and meta-analysis. Clin. Nutr. ESPEN, 41, 59–67.
78 Mousavi, S. M. et al. (2019) Resveratrol supplementation significantly influences obesity measures: A systematic review and dose-response meta-analysis of randomized controlled trials. Obes. Rev., 20, 487–498.
79 Tabrizi, R. et al. (2020) The effects of resveratrol intake on weight loss: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr., 60, 375–390.
80 Clasen, B. F. et al. (2014) Growth hormone signaling in muscle and adipose tissue of obese human subjects: Associations with measures of body composition and interaction with resveratrol treatment. J. Clin. Endocrinol. Metab., 99, E2565−E2573.
81 Konings, E. et al. (2014) The effects of 30 days resveratrol supplementation on adipose tissue morphology and gene expression patterns in obese men. Int. J. Obes. (Lond.), 38, 470–473.
82 Cottart, C.-H., Nivet-Antoine, V. & Beaudeux, J.-L. (2014) Review of recent data on the metabolism, biological effects, and toxicity of resveratrol in humans. Mol. Nutr. Food Res., 58, 7–21.
83 Lin, C.-T., Sun, X.-Y. & Lin, A.-X. (2016) Supplementation with high-dose trans-resveratrol improves ultrafiltration in peritoneal dialysis patients: A prospective, randomized, double-blind study. Ren. Fail., 38, 214–221.
84 Shaito, A. et al. (2020) Potential adverse effects of resveratrol: A literature review. Int. J. Mol. Sci., 21, 2084.
85 Resveratrol (2021) naturalmedicines.therapeuticresearch.com https://naturalmedicines.therapeuticresearch.com/databases/com.